
Preventing, Predicting and Alleviating Pain at Stanford
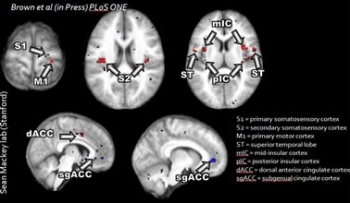
An image of the brain as pain is registered.
According to the 2011 Institute of Medicine's Relieving Pain in America Consensus Report, 100 million people in the U.S. suffer from chronic pain. That is nearly one out of every three people. Yet no two individuals experience pain in quite the same way. The highly subjective and personalized nature of pain make it a complex problem to diagnose and treat.
Understanding how to predict, prevent and alleviate pain remains the mission of the Stanford Division of Pain Medicine, according to Division Chief Sean Mackey, MD, PhD. In the last decade, he has seen dramatic changes in the way pain is understood. Rather than viewing pain as simply a symptom of trauma, infection, inflammation or surgery, pain specialists like Mackey now see it as a discrete disease entity — one that fundamentally alters the entire nervous system. Advanced neuroimaging tools have allowed them to peer inside the brain, unlocking mysteries of where pain is perceived and processed, how it affects the brain and how it can act to change thoughts and emotions.
"For the first time, we have the tools to effectively explore the impact of pain on the brain," says Mackey. "And we can use this information to create the comprehensive interdisciplinary treatment needed to prevent or reverse these changes."
Stanford tests objective pain-o-meter
Although pain is a major symptom and indicator of many illnesses, physicians must currently rely on their patients' subjective self-reporting to measure pain. "One of the key things we have all been searching for is an objective way to determine whether a person is in pain or not," says Mackey. "There are huge individual differences in how people experience pain, and it’s not directly correlated to the extent of the injury."
In a study published last year, Mackey tested a method of analyzing brain structure using advanced computer algorithms that accurately predicted whether a patient had lower back pain 76 percent of the time. Mackey's team used a machine-learning approach to perform the study. Using these pattern classifiers, the same type of algorithms used by Google in its search engine, Stanford researchers were able to find patterns of brain activity and brain structure that correlate and predict the experience of pain.
"This method may one day augment self-reporting as the primary way of determining whether a patient is in chronic pain," says Mackey, professor of anesthesiology, perioperative and pain medicine, and neurosciences and neurology (by courtesy).
Genetics play a role in pain treatment
And just as individuals experience pain differently, how patients respond to pain treatment is also highly variable and genetically predestined, according to a separate study by Martin Angst, MD, professor of anesthesia. Although opiates remain the mainstay medication for easing pain, they don’t work well for everyone because of side effects. The Angst study showed that genetics play a significant role in determining which patients will suffer the most from disturbing side effects of opiates such as nausea, slowed breathing and dislike for a drug.
Gaining a better understanding of these genetic differences may change how physicians administer medications and treat patients with pain.
Using the mind to alleviate pain
In a new treatment method being tested at the Pain Center, researchers are using real-time functional magnetic resonance imaging (fMRI) neuro-feedback to manipulate brain activity. Unlike biofeedback, which involves monitoring and manipulating downstream processes such as heart rate or temperature, Mackey’s team is going directly to the brain systems involved in the experience or modulation of pain and increasing or decreasing those. Patients can learn how to control their own brain systems with profound effects on their pain, he says.
"We can focus on any brain region or pattern of brain activity, and feed that back to patients so they can learn to control their brain in real time,” says Mackey. "It's like working on a muscle at a gym, but you’re working on your brain."
In other mind-body research, the NIH has provided Stanford with a $10 million grant for research on understanding the mechanisms of four treatments for low back pain —real-time fMRI neuro-feedback, mindfulness-based stress reduction, cognitive behavioral therapy and acupuncture.
"Patients' beliefs and emotions play at least as much of a role in the amount of pain they experience and their disability as anything else," says Mackey. "We hope to one day take into account a patient’s unique, neurobiologic and genetic makeup, the injury the patient sustained and the amount of pain they are in, and with a high degree of accuracy, be able to predict what treatment is most likely to work for that patient. "Our goal is to one day create a personalized pain management approach."
By Grace Hammerstrom