
Zeroing in on Concussions
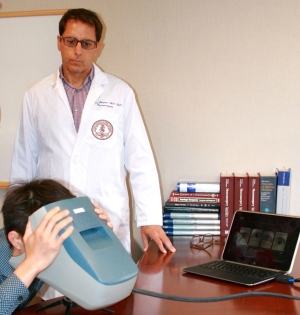
Jamshid Ghajar, MD, uses the eye-tracking technology he developed to record a patient's eye movement for 30 seconds as a way of diagnosing concussions more accurately and tracking recovery.
December 2014
Diagnosing and treating concussions is an inaccurate science at best. There is presently no evidence-based definition for concussion that is uniformly applied in clinical and research settings. And there is extreme variability among clinicians on how concussion is diagnosed and managed. The Stanford Concussion and Brain Performance Center, a specialized center to diagnose and treat patients who experienced a recent concussion, is hoping to bring clarity to this concussion conundrum.
With no standard test or procedure to verify whether a patient has had a concussion, its diagnosis is based on a doctor's examination, observation of symptoms, testing a patient's reaction time and memory and understanding the incident that led to the injury. But according to Jamshid Ghajar, MD, PhD, Clinical Professor of Neurosurgery and Director of the Stanford Concussion and Brain Performance Center, clinicians are not looking at the right predictors for concussion when they rely on symptoms or memory and reaction tests. Predictive movement, he says, is a more accurate sign of concussion.
"When the brain's timer, the cerebellum, is rattled, it affects both motor and thinking pathways," says Ghajar, who is also president of the Brain Trauma Foundation. "That's why patients who've suffered a concussion feel out of sync. When somebody gets out of sync in their thinking, they also get out of sync in their movements."
When a patient is evaluated at the Stanford Concussion Center, physicians have them walk on a treadmill and can pick up jitteriness and instability by looking at patients' step-to-step variability and balance. They also measure their attention or cognitive focus using a new neuro-technology device developed by Ghajar, which tracks a patient's eye motion for 30 seconds. Patients place their face in the eye-tracking device and are then asked to follow a dot as it rotates around a circle. The patient's gaze is measured against his or her baseline movement or against a normative database. Eye-tracking has been shown to correlate strongly with the integrity of the attention network, which is commonly impaired in concussion.
"We can actually measure the problem, compare data to normal and try to improve upon it," says Ghajar. "This differentiates us from any other concussion clinic in the world because of the diagnostics we're doing and the therapeutics we offer that really give patients a solution."
Tracking recovery
Because people who have suffered one concussion are three times more likely to get another concussion, usually because they resume activity when still suffering from attention and motor issues, it is critical to be able to measure recovery, says Ghajar. Using eye-tracking technology, he and his colleagues can regularly retest patients post concussion to track their recovery as a more accurate way of determining when it's safe for them to resume activity.
Patients who've suffered a concussion feel out of sync. When somebody gets out of sync in their thinking, they also get out of sync in their movements.
In two studies Ghajar is conducting on behalf of the Department of Defense, he is collecting baseline eye-tracking readings of 5,000 athletes in the Bay Area and on the east coast, as well as 5,000 soldiers at Fort Hood to establish normal eye tracking values and to assess eye tracking after a concussion.
"Of those groups, about five to ten percent will end up with a concussion," says Ghajar. "So we will be able to follow them and do eye tracking on them again if they suffer a concussion." These baseline measurements will allow Ghajar to compare the patient's normal reading with the reading post concussion, and establish a set target to reach in recovery.
Active treatment prescribed
The Stanford Concussion Center also offers an active treatment protocol that goes beyond the standard rest that physicians have prescribed in the past. Physicians at Stanford work to improve patients' balance, walking and eye movement through exercise and feedback to regain executive function quicker and recover sooner. The thrust behind the clinic is that by treating movement problems, patients' timing gets better and their thinking improves, says Ghajar.
Patients who come to the Concussion and Brain Performance Center are evaluated by one of three neurologists or neurosurgeons—Ghajar, Jaime Lopez or Viet Nguyen. At the same visit, they meet with a physical therapist for balance and movement testing and therapy, and they receive a neuro psych evaluation. Patients will then get rehabilitation in the areas where they are experiencing deficits. The orthopedic department works closely with the Clinic to do the assessment and treatment of movement problems.
The School of Medicine has also been enlisted by the federal government to establish evidence-based guidelines to standardize and improve on the huge variability in diagnosis and treatment of concussions. To date, the effort led by Ghajar and Nancy Carney, PhD, Research Director at the Brain Trauma Foundation and investigator at Oregon Health & Science University, has identified four "prevalence indicators" of concussion, which are completely evidence-based. They are: disorientation or confusion immediately after the event; impaired balance within one day after injury; slower reaction time within two days after injury; and impaired verbal learning and memory within two days after injury. They published these results inNeurosurgery and will be updating those results with concussion diagnostic criteria and prognosis in the coming year.